soleceismical
soleceismical t1_j43eppn wrote
Reply to comment by GlitteringVersion in TIFU by jokingly telling my friend he was born on a laboratory by JJJJPPPPP8A
Imagine what a massive change it would be if babies could actually be gestated and born in a lab. How much it would reduce pregnancy-related death and disability. And the abortion debate would be moot because they'd just stick those suckers in an artificial womb instead.
soleceismical t1_ius4mu4 wrote
Reply to What does a muscle knot look like? by annieca2016
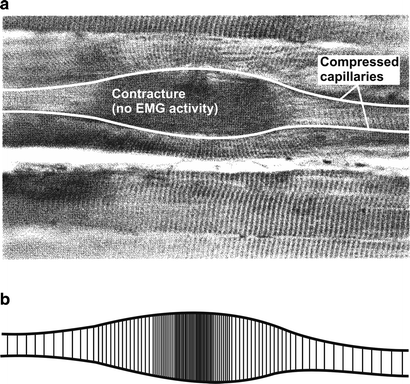
It's believed to be a small segment of sarcomeres near where the nerve penetrates the muscle that are stuck in contraction, perhaps because there is inflammation impeding the flow of blood to the area to remove waste products and deliver oxygen to feed the Krebs cycle and provide the ATP needed to break the cross bridge between the actin and myosin. It can be due to sedentary lifestyle, muscle strain, poor posture, or a combo like being sedentary and then trying to do things you used to be able to do five years ago without working back up to it.
To treat them, you can massage them out with a theracane or yoga balls or a licensed masseuse trained in myofascial release. If you have greater problems/pain, you may want to see a physical therapist (especially one with FAAOMPT or similar credentials). You'll want to stretch and move the muscles through their entire range of motion. Increase physical activity and weight gradually instead of trying to lift a couch one weekend when you've done no lifting in a while. Get a computer setup that is ergonomically appropriate. Most people need to work out their mid and lower traps and glutes and abs.
{kind=link}
Here's some photos and a drawing of what they are supposed to look like:
{kind=link}
More info:
>A Trigger Point (TrP) is a hyperirritable spot, a palpable nodule in the taut bands of the skeletal muscles' fascia. Direct compression or muscle contraction can elicit jump sign, local tenderness, local twitch response and referred pain which usually responds with a pain pattern distant from the spot[1][2][3][4].
[...]
>Anatomy and Etiology
>Trigger points develop in the myofascia, mainly in the center of a muscle belly where the motor endplate enters (primary or central TrPs)[5]. Those are palpable nodules within the tight muscle at the size of 2-10 mm and can demonstrate at different places in any skeletal muscles of the body. We all have TrPs in the body. Can be present even in babies and children, but their presence does not necessarily result in the formation of pain syndrome. When it happens, TrPs are directly associated with myofascial pain syndrome*, somatic dysfunction, psychological disturbance and restricted daily functioning[7].
[...]
>Causes - Usually, TrPs happen due to:
> *Ageing,
> *Injury sustained by a fall, by stress or birth trauma.
> *Lack of exercise - commonly in sedentary persons between 27,5-55 years, of which 45% are men[9],
> *Bad posture - upper and lower crossed pattern, swayback posture, telephone posture, cross-legged sitting,
> *Muscle overuse and respective micro-trauma - weightlifting,
> *Chronic stress condition - anxiety, depression, psychological stress trauma,
> *Vitamin deficiencies - vitamin C, D, B; folic acid; iron;
> *Sleep disturbance,
> *Joint problems and hypermobility.
>Pathogenesis and Theories
>Little is known about the formation of TrPs. There are some theories written in literature who try to explain the formation, sensitization, and manifestation of TrPs, but few of them have strong evidence[3][10][11].
>Under normal conditions, pain from TrPs is mediated by thin myelinated (Ad) fibers and unmyelinated (C) fibers. Various noxious and innocuous events, such as mechanical stimuli or chemical mediators, may excite and sensitize Ad fibers and C fibers and thereby play a role in the development of TrPs.
>Integrated Trigger Point Hypothesis (ITPH) is the present working hypothesis. When sarcomeres and motor endplate become overactive for a number of different reasons, pathological changes start at cellular levels. This turns on permanently sarcomeres leading to a local inflammatory response, loss of oxygen supply, loss of nutrient supply, endogenous (involuntary) shortening of muscle fibers, and increased metabolic demand on local tissues.
>Electrophysiological investigations of TrPs reveals phenomena which indicate that the electrical activity arises from dysfunctional extrafusal motor endplates rather than from muscle spindles[12].
>Polymodal theory explains the existence of polymodal receptors (PMRs) throughout the body which under certain constant, pathological stimuli turn into trigger points[13].
>Radiculopathic theory explains direct relationship between problems on nerve roots which lead to local and distant neurovascular signals and trigger points creation[14].
>Peripheral and Central Sensitization - Central sensitization is a phenomenon, together with peripheral sensitization, which helps in understanding chronic or amplified pain. There is central sensitization after an intense or repetitive stimulus of the nociceptor present in the periphery, leading to a reversible increase of excitability and of the synaptic efficacy of central nociceptive pathway neurons. Manifested as hypersensitivity to pain (called tactile allodynia and hyperalgesia secondary to puncture or pressure). These CNS changes may be detected by electrophysiological or imaging techniques[15][16].
soleceismical t1_iufs0vp wrote
Reply to comment by beyd1 in LPT: Try to keep problems with you and your significant other between the two of you. by Pale_Perception_4927
People will remember that you keep having fights and they wish you wouldn't keep making up. If it's an isolated incident that gets permanently resolved, they will forget it.
soleceismical t1_iufrfas wrote
Reply to comment by Fun_Amount3063 in LPT: Try to keep problems with you and your significant other between the two of you. by Pale_Perception_4927
Damn OP is spiraling HARD. Maybe he should have talked to his own friends (and not hers) about the relationship. But it just sounds like she is not at all interested and that's why she ended it. I hope he can get support and distraction from his own IRL friends and family to help him move forward.
soleceismical t1_iufpkpp wrote
Reply to comment by cptwott in LPT: Try to keep problems with you and your significant other between the two of you. by Pale_Perception_4927
Just note that you are not supposed to get couples counseling if there's any kind of abuse, including of the emotional or psychological variety.
https://www.thehotline.org/resources/should-i-go-to-couples-therapy-with-my-abusive-partner/
soleceismical t1_j859xum wrote
Reply to comment by TheAmazingDuckOfDoom in Wedding Planner in Ukraine War Has Adapted to Curfews, Blackouts, the determination to keep on living and to be happy is so heartwarming. by TheHuanWhoKnocks
If they are doing it to protect their loved ones, it sounds like love is the primary incentive.