Submitted by tonymmorley t3_ypx6jz in Futurology
Comments
JohnABurns t1_ivnn2oh wrote
Sounds promising.
brockclarke t1_ivo7qks wrote
Technically it’s the dose RATE that’s key here
Mounta1nK1ng t1_ivpfdpt wrote
Dose rate, and all delivered in a single pulse.
Mounta1nK1ng t1_ivlmclz wrote
This is interesting, but we don't usually see any side effects when treating bone mets in the limbs as the surrounding tissue isn't all that radiosensitive. The next study will tell us a lot more.
ptjunkie t1_ivnun4u wrote
This proton therapy system isn’t really intended for limbs. It specializes in sensitive areas where you need the radiation dose to penetrate the skin, but not exit the other side of the body. Typical uses are ocular, brain, and prostate.
I suspect that they are just testing this FLASH delivery on less sensitive areas before they blast someone in the head with it.
Mounta1nK1ng t1_ivpaqay wrote
I was looking in the article to see whether it was a photon or proton based system, since you can do FLASH with both, but I must have missed it. I understand it's not intended for limbs. We already do palliative treatments in one fraction with little to no side effects.
[deleted] t1_ivnt6qf wrote
[deleted]
17FeretsAndaPelican t1_ivlofrs wrote
Call me a pessimist but I am 32 years old and I cannot remember a year going by when the news said a new amazing cancer treatment massively suceeded jn trials and then we never heard about it again. And then the amount of people dying of cancer went up.
sault18 t1_ivloyj1 wrote
Cancer survival rates have been improving for decades.
InSight89 t1_ivlscx5 wrote
>Cancer survival rates have been improving for decades.
That's not really in question. Improvements in health and cancer treatments have definitely improved.
But I agree with the OP. It's the periodical headline of "New treatment may cure cancer" nonsense that seems to go nowhere. It's great that they are trying their best. But I feel like it provides a lot of people with false hope.
Having had two relatives die from cancer, one of them in a fairly horrendous way and whom begged to be a participant in such trials, seeing headlines like this is nice but I generally don't give them much thought anymore beyond reading the comments section.
[deleted] t1_ivltpuc wrote
The problem is with the reporting.
im_thatoneguy t1_ivlr1fy wrote
{kind=link}
must_decide t1_ivmahlq wrote
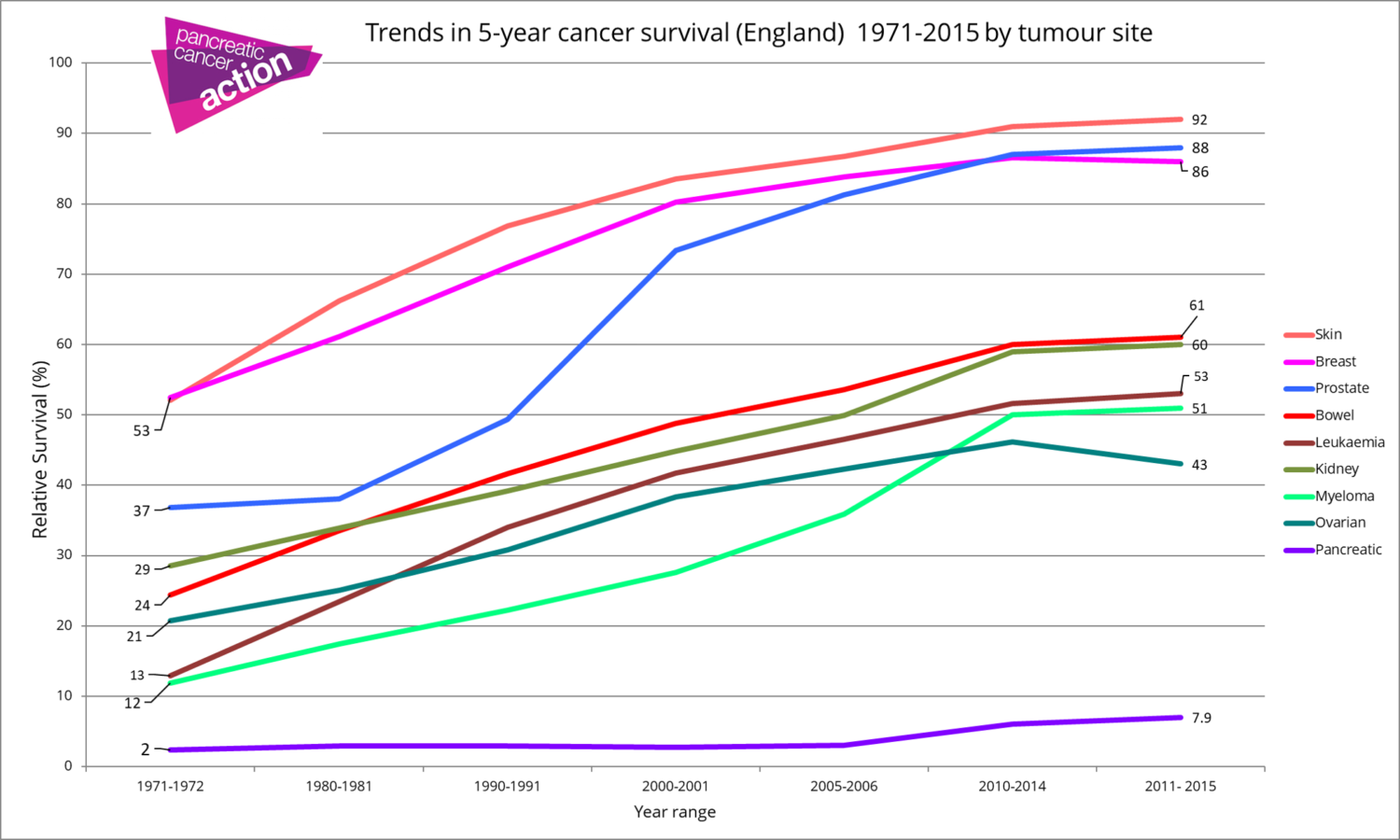
Very interesting graph! What an improvement in some survival rates in just the last decade even, but I’m curious what could be the reasons for the decline in survival rate for ovarian cancer?
And wow, pancreatic cancer… brutal!
Lisagreyhound t1_ivnypwq wrote
The brca genes are both for breast and ovarian cancers. Detection of ovarian cancer is still terrible. So perhaps women with a brca gene survive BC but then get ovarian cancer? (A total guess).
su_baru t1_ivmn7p4 wrote
The oncology sector has the most new drugs approved each year, each of them being approved on the basis of adding some benefit over traditional regimens. The improvements may seem minor with each new drug approval but the net effect over many years is drastically improved cancer outcomes.
17FeretsAndaPelican t1_ivrdshj wrote
I hear you. But I watched my mum die in 2003 (not looking for sympathy) and a few months ago I watched blow for blow the same thing happen to someone else like it was an action replay. I'll believe it when I see it. Until then I'm just gunna donate to cancer research and ignore it until I have to go through it like most people.
su_baru t1_ivtwgid wrote
I’m sorry to hear that. I’m sure my previous comment provides no comfort when you see it happen to friends and family.
17FeretsAndaPelican t1_ivut78i wrote
I also don't want people to think I'm discounting the incredibly hardworking researchers and doctors fighting tirelessly to save lives. They do absolutely everything they can.
I'm just whinging.
Mavman11 t1_ivmbvjs wrote
I agree with you. I feel like I see an article like this once a week and we've still been using the same treatment methods for years
Mounta1nK1ng t1_ivphc1n wrote
Amount of people dying of cancer went down despite people continuing with behavior that increases cancer like smoking, being overweight, not eating enough fruits and vegetables, and eating too much processed meat.
We're better at detecting it now, and better at treating it.
Also people overly hype mouse trials to get funding, but humans are not mice. The results frequently don't translate well.
herrkuchenbaecker t1_ivpux9d wrote
I say
FLASH Ah-ah It'll save every one of us!
PartyPineapples714 t1_ivlhf9v wrote
Interesting. Are there any published journals on this yet?
ReasonablyBadass t1_ivnskp7 wrote
I never quite got why we don't use multiple radiation beams from multiple angles?
Low powered in the tissue they pass, but overlapping in the tumor.
TheFram t1_ivo5wkf wrote
We do. There are various techniques used to deliver modern radiation treatments and they rarely use only a single beam to treat a tumor. That only really happens for skin lesions. Otherwise, multiple-beam radiation therapy techniques include 3D conformal , IMRT (intensity modulated radiation therapy), DCA (dynamic conformal arcs), VMAT (volumetric modulated arc therapy), SBRT (stereotactic body radiation therapy)….the list goes on.
There are many factors involved in choosing a technique such as exit dose (radiation dose to tissue beyond the target), skin dose, (maximum dose is not at the point of beam entry on skin but rather at a calculated depth), treatment site, treatment intent (palliative patients typically get insurance approval for less-conformal treatment plans since the dose to surrounding areas is lower than a curative dose which is much more aggressive), etc.
Source: I am a radiation therapist, AKA the person who delivers the treatments.
ReasonablyBadass t1_ivo63q5 wrote
Ah cool, thank you!
rysvel t1_ivo1f13 wrote
Look up SBRT
Egoy t1_ivohqvy wrote
Already answered but I wanted to put it in layman’s terms in case anybody was wondering. When they do even and ‘old school’ x-ray rad treatment the beam is rotated around multiple axis centred on the treatment location. The tech line up your markings to put the treatment location at the correct spot the.n the machine rotates With another rotating head on it as well so the beam path hits different tissue during the treatment except at the treatment location. Surrounding tissue gets a significantly lower dose than the target location.
I did 25 rounds in 2021, it’s crazy how sophisticated even the outdated treatment methods are.
ptjunkie t1_ivnstho wrote
They do, but typically the delivery nozzle of the machine rotates around the patient to get other angles.
ReasonablyBadass t1_ivnt9d7 wrote
I meant at the same time, so that you get higher energy in the tumor tissue.
ptjunkie t1_ivntufc wrote
I don’t think there is a benefit from doing it all at once. You can just rotate and dynamically collimate the beam to hit it over a longer period of time with the same effect.
Not to mention that multiple angles would require multiple beams, or complicated beam splitters to change the energy levels for the changing depth of tumor from different angles.
In practice, most treatment plans are delivered in fractions anyway, to synchronize the radiation delivery with the cancer cell life cycle.
They aren’t trying to burn the tumor out, they are trying to snuff out the tumor cells as the body heals around it.
st4nkyFatTirebluntz t1_ivnxe2o wrote
Listen, I'm high, tired, and didn't even slightly read the underlying study. But, wasn't that the whole point? That they tried maximizing the rate of delivery to the affected area, and that it seems to improve the ratio of therapeutic benefit to harmful side effect?
Spitballing wildly, I'd imagine there's some sort of optimal rate for tumor destruction (obviously dependent on the type of tumor and other specific details), and optimal rates for non-tumor preservation, and you'd be able to optimize between the two by utilizing multiple beams from multiple directions in certain scenarios.
Mounta1nK1ng t1_ivpfm3h wrote
You are correct. The whole point is delivering it all at once so you get the FLASH effect. Different radiobiological mechanism than traditional fractionated radiotherapy.
Mounta1nK1ng t1_ivpcbmz wrote
The FLASH studies have shown the lower side effects by using a single pulse, so the idea when putting this into clinical practice would be a single shot. Obviously no fractionation, as this isn't relying on the 5 R's. It's relying on a transient radiation-induced hypoxia that affects tumor cells more as they're already hypoxic.
For clinical treatment they would be looking at multiple treatment head gantries so the tumor could be shot from multiple angles at once in a single pulse so that you get the benefit of the FLASH effect that this treatment relies on.
Xist3nce t1_ivntq00 wrote
Interesting point. Now I wonder that too. It’s so simple so there’s got to be a reason, maybe it’s just not effective? Any cancer researchers wanna chime in to sate this curiosity?
TheAero1221 t1_ivo99i1 wrote
REFER TO GUY BELOW
Not a researcher, but I know that traditionally there has been a concerted effort to deliver radiation to the cancer site via small angles of attack that vary over time. They do this because even though the radiation is not at its maximum concentration when traveling through the noncancerous tissue, there is still some chance of causing undesired damage if those areas are repeatedly exposed. Subsequent treatments change the angle of attack so that they can minimize the radiation exposure to any given area of tissue that they do not wish to damage. Attacking from a wider angle may mean less total safe treatments are possible since fewer viable attack angles will remain after each treatment. Idk. Again not a researcher, just guessing. Could be totally wrong.
Mounta1nK1ng t1_ivpj6t8 wrote
You are correct that you're totally wrong. We don't vary the angles over time, we just select a large number of angles. Basic idea, if you shot from just one angle, all the tissue on the entrance path would be getting more dose than the tumor. If you shot through 10 different angles for a single treatment, than each entrance path through normal tissue would be getting only 10% of the dose, but where they all overlap at the tumor, it's getting 100% of the dose. This treatment with the 10 angles (usually actually only 5, 7, or 9 for static IMRT) would be given every day for 5-8 weeks in conventional radiotherapy using those same angles for each daily treatment.
The evolution of this is having the gantry rotate constantly through the treatment, varying the dose rate and shape of the beam during the rotation to avoid dose to especially sensitive tissues, while making sure you completely cover the target. So instead of 10 (or 5 or 7) discrete angles you have the maximal spread of the entrance dose. It's called VMAT, volumetric modulated arc therapy.
FuturologyBot t1_ivlgvv4 wrote
The following submission statement was provided by /u/tonymmorley:
>"It delivers a dose of radiation that’s over 300 times higher than traditional radiation therapy in just a fraction of a second. This induces something called the “FLASH effect” — a not-entirely-understood phenomenon in which the radiation still attacks the tumor, but doesn’t harm surrounding tissue."
​
>"Ultimately, the researchers believe FLASH radiotherapy would be most useful for treating cancers in the brain, lungs, or gastrointestinal area, as the tissues around those tumors are particularly vulnerable to damage from traditional radiation therapy."
Please reply to OP's comment here: https://old.reddit.com/r/Futurology/comments/ypx6jz/experimental_flash_cancer_treatment_aces_first/ivlb1up/
[deleted] t1_ivlqbsv wrote
[removed]
[deleted] t1_ivm0x7f wrote
[removed]
[deleted] t1_ivmdm00 wrote
[removed]
[deleted] t1_ivmfhgv wrote
[removed]
[deleted] t1_ivmr4ab wrote
[removed]
[deleted] t1_ivnrp7e wrote
[removed]
[deleted] t1_ivnsljq wrote
[removed]
[deleted] t1_ivo0p22 wrote
It makes me wonder if corrupted DNA and tissue has different thresholds for triggering apoptosis or different properties that make it susceptible to things like this that wont damage the rest of you.
norby2 t1_ivs0s83 wrote
That’s been one theory floating around for a bit.
el_goate t1_ivoc9q9 wrote
This, like cyberknife radiation therapy(sbrt) , will likely only be usable for early stage tumors with no lymphatic spread. Cyberknife is not really a reliable treatment. So many with recurrence, progression etc and is mostly used for frail patients who can’t tolerate surgery. Surgery with lymph node dissection is still the best chance at cure.
NCFlying t1_ivoo6ec wrote
Does this use existing technology/machines or are we looking at special updates capex intensive machines to provide these dosing levels?
[deleted] t1_ivopnr0 wrote
[removed]
[deleted] t1_ivpupx0 wrote
[removed]
[deleted] t1_ivlhva7 wrote
[deleted]
tonymmorley OP t1_ivliabr wrote
Did you open the op-ed before commenting? 🤔
tonymmorley OP t1_ivlb1up wrote
>"It delivers a dose of radiation that’s over 300 times higher than traditional radiation therapy in just a fraction of a second. This induces something called the “FLASH effect” — a not-entirely-understood phenomenon in which the radiation still attacks the tumor, but doesn’t harm surrounding tissue."
​
>"Ultimately, the researchers believe FLASH radiotherapy would be most useful for treating cancers in the brain, lungs, or gastrointestinal area, as the tissues around those tumors are particularly vulnerable to damage from traditional radiation therapy."