BeneficialWarrant
BeneficialWarrant t1_je0u159 wrote
Reply to ELI5: if protein is broken down into peptides in the stomach/digestive tract, why would consuming something like "active collagen" do anything? by Alexander_Elysia
OP asking the right questions. The main effect of oral collagen supplements is that they can build healthy, full, and radiant portfolios for the supplement makers. The "glow" of having money is very noticeable.
BeneficialWarrant t1_jdu0rmz wrote
While I don't know the full answer, I can assure you that motor deficit does occur with even mild mixed peripheral nerve compression. Weakness and muscle atrophy is a hallmark sign of nerve entrapment, although I agree that sensory effects often seem more immediately noticeable.
Perhaps unconscious proprioceptive feedback circuits modulate motor tone to compensate for mild weakness and ensure normal posture. Or perhaps somatosensory deficit is more bothersome and therefore more consciously noticeable. Or perhaps it has to do with a difference in fiber physiology or myelination. I'd guess it has more to do with the first 2, and its simply that the body is more consciously aware of sensory deficit while mild motor deficit is handled more unconsciously.
Edit: As another person pointed out, the correct answer is that sensory fibers are conveyed around the periphery and motor towards the center of the nerve. Appreciate the love though. I tried my best.
BeneficialWarrant t1_jdsk5c1 wrote
Reply to ELI5: How is there enough water pressure to delivery water to every home and apartment in a city? by Maxweilla
One of the nice things about a water tower is that the pressure is not really affected by flow rate (unlike a traditional pump which has a limited power output and where the pressure drops off as flow rate increases).
Potential energy is stored in the tower. If more people turn on the tap, the potential energy just gets used faster. So long as the tank doesn't run dry, there will always be water pressure for everyone. Then a pump can slowly supply the tower during times of low use such as nighttime.
BeneficialWarrant t1_jdrx8pt wrote
There are many factors that go into choosing dosing intervals. Some drugs are described as "bactericidal" vs "bacteriostatic". Some bactericidal drugs have a "concentration-dependent" response rather than a "time-dependent" response, which means that they are more effective when given a large dose for a short duration rather than a smaller dose for a longer time. Some drugs also continue to inhibit bacterial growth even when it is no longer detectable in blood (postantibiotic effect)
There is a class of drugs called aminoglycosides (tobramycin, streptomycin, amikacin) that are often taken at long intervals. They have an initial concentration-dependent bactericidal effect when first taken, then continue to provide bacteriostatic effect for many hours. Infrequent dosing also helps reduce toxic side-effects (hearing damage).
Also drug makers try to make drugs which can be taken as infrequently as possible while still being effective in order to improve patient compliance. They want you to take the drug as directed and not create a resistant super-bug. If the drug is effective when only taken once or twice per day, particularly in oral medication for an outpatient, this is preferable to a drug that is taken multiple times per day. Its just human nature to forget a dose here or there and to be less motivated to remember doses on time once you start feeling better.
BeneficialWarrant t1_jbziikc wrote
The answer is sort of both.
The cell has its perikaryon (body) in the hypothalamus (supraoptic nucleus) and axonal extensions in the posterior pituitary. So its inside of a cell of the supraoptic nucleus but its in the region called the posterior pituitary
Neurons are often quite long and synthesize neurotransmitters (or neurotransmitter precursors) in one area but then transport them intracellularly to a target area.
BeneficialWarrant t1_j9uwe3q wrote
Reply to comment by RuhrowSpaghettio in when a limb gets amputated, how do they stop the flow of blood? by EnchantedCatto
OK, prior caveat: This will be a long post and will not directly cite publications for every claim
So first off, I'll say that my advice on the topic is informed by (but not infringing on any intellectual property) my time working as a 911 dispatcher using data-informed protocols for prehospital treatment by laypeople (created by a Salt Lake City-based organization that is generally recognized as the standard for these protocols, and which sells them to most public-safety emergency answering centers.) [Bohm and Kurland, 2018] While this raises doubts about its accuracy, it establishes its uniquity] I understand that instructions for tourniquet use by non-healthcare personnel is changing as newer data shows that, as you said, improperly applied tourniquets are not as harmful as once believed and that laypeople can apply tourniquets effectively and quickly with proper instruction. [Scott, et. al. 2020] I believe that the previously mentioned company may have altered their product to reflect this, but I've been out of that gig for a few years now.
That said, the reason why (at the time) laypeople were generally not advised to apply tourniquets in the absence of unambiguously lethal, uncontrollable hemorrhage was not that a poorly applied tourniquet could worsen the outcome for a person with an otherwise lethal hemorrhage. Instead, it was to discourage the use of tourniquets when not necessary, as it was believed that a layperson may not be able to make this distinction and thus use them excessively. The vast majority of prehospital appendicular bleeds probably do not require tourniquet use (anecdotal, but it was probably close to 1 in 100 during my time answering phones). This is probably due to the low threshold some people have for requesting emergency medical transport. For a layperson who may have trouble telling the difference, attempting to control bleeding by direct pressure first is often a good idea in the absence of unquestionably uncontrollable, arterial (or massive venous/tissue capillary bed) hemorrhage.
TLDR: Until recently, tourniquet use by untrained laypeople was generally discouraged, but things have changed within the past few years.
BeneficialWarrant t1_j9fwl00 wrote
Reply to comment by baggier in How did we first figure out which substances are elements and which are compounds? by sapphics4satan
But if you heat up some of these so-called elemental metals in air, they combust, releasing phlogiston, which is comprised of elemental fire. Hypothesis busted! Q.E.D.
BeneficialWarrant t1_j9e6uto wrote
Reply to comment by davtruss in when a limb gets amputated, how do they stop the flow of blood? by EnchantedCatto
Its debatable whether an untrained person could help more than harm by applying a tourniquet. Some sources say yes, some say no. If you are familiar with how it works and there is uncontrollable bleeding from an appendage, then yes, wind that sucker down tight.
Edit is to reflect more up-to-date instruction. You can see discussion in below comments for context.
Tourniquet use is appropriate for a bleed from a limb which cannot be controlled by direct pressure alone. Without training or instruction, an improvised tourniquet applied by a layperson isn't likely to be effective. Fortunately, proper tourniquet use can be learned in only a few minutes and an emergency services dispatcher can instruct you on tourniquet use if you find yourself in a situation where it is necessary and you don't know how to do it. If in doubt and the patient is conscious, it may be a good idea to first attempt to control bleeding with direct pressure alone. Note that direct pressure is not appropriate if there are significant amounts of sharp, foreign bodies within the wound which may make the injury worse than it already is. In that case, elevation, manual arterial compression, and tourniquet use as needed will be the appropriate first-aid.
Tourniquet or not, you can help by finding a clean and dry cloth, garment, towel, applying firm pressure, and don't remove the cloth. If it bleeds through, put another cloth on top and keep the pressure on! You can also apply pressure to the artery above the bleed. Groin for the leg and under the biceps for the arm.
Don't remove any foreign object that may be sticking out of the person, don't put yourself in danger that might cause a second casualty, and don't move a patient who may have suffered a spinal trauma unless absolutely necessary.
BeneficialWarrant t1_j9b4rem wrote
Reply to Why are we not acidic? by stronkreddituser
1: Amino acids contain both an organic acid and organic base.
2: The acid and base are both neutralized in the process of making a protein.
3: Some amino acids remain acidic or basic after becoming part of a protein because of extra parts they have on a side chain (sort of like a pendant or charm hanging down from a necklace).
4: Excess acid in the body is is neutralized by carbonate which can then be converted to CO2 and exhaled or filtered out by the kidneys into urine. There is baking soda in your blood and you can't survive without it.
BeneficialWarrant t1_j9823fl wrote
Reply to comment by buddhistbatrachian in Do arthropods experience emotions and/or pain, and how can we know that? by _Marteue_
I'm sorry, I only remember reading about a complete C. elegans simulation with 302 neurons several years ago and assumed that more advanced simulations have since been run. I actually don't know for sure and haven't looked into it since. I apologize if that was misleading.
BeneficialWarrant t1_j9746la wrote
As far as I'm aware, we don't have a good way of objectively describing, measuring, or comparing a subjective "experience". We know that they can detect a nociceptive (painful) stimulus and change their behavior to avoid the stimulus. We can even accurately simulate the entire nervous system of some simple arthropods in a computer program and completely understand how they process information and "think". Despite this, I don't think we can know if they suffer.
BeneficialWarrant t1_j5ft3vx wrote
No, an allergic reaction requires circulation. The perfume might diffuse into tissue and activate a few surviving mast cells, but the vasoactive chemicals (cytokines and biogenic amines) would have no real effect. Every sustained immune response I can think of requires recruitment of other cells (through circulation). Some tissue-resident phagocytes could maybe become activated through passive diffusion (although this is much less likely without circulation), but any effect they have would be *far* less damaging than the enzymatic reactions already taking place in tissue after death.
BeneficialWarrant t1_j5fm1b3 wrote
All the speaker does is move forwards and backwards. Its a linear motor.
If you take 2 signals (say 2 simple frequencies) and add them together, you get a new, combined signal.
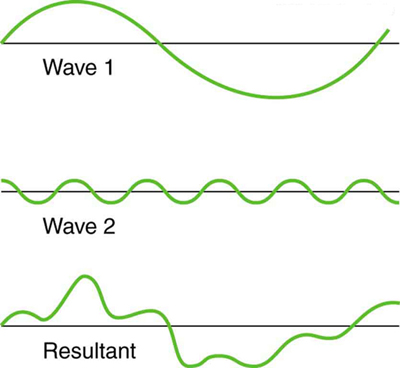{kind=link}
The above combined signal is created from 2 simple sine waves with a high and a low frequency. If the speaker moves in the combined pattern, it will create waves of air pressure which will stimulate 2 different length hair cells in your cochlea.
BeneficialWarrant t1_j5fcjkp wrote
Reply to comment by Old-Advice-5685 in Would it be possible to modify a virus to target cancer cells? by KetogenicKraig
There are surface biomarkers which are upregulated in certain cancers. CD155 in glioblastoma is an example.
Also, plenty of mechanisms for regulating death and division are on the surface. Growth factor receptors, apoptotic receptors, matrix attachment proteins. Yeah, lots of oncogenes code for membrane proteins. The houses do not all look the same.
BeneficialWarrant t1_j477q57 wrote
Blood types can be visualized under a light microscope if IgM antibodies are added to the blood. This is a very fast and easy way to determine blood type. What you actually see is the blood cells clumping together (the actual A, B, and Rh proteins are far too small to be seen except perhaps by very specialized equipment).
​
{kind=link}
BeneficialWarrant t1_j28y8gq wrote
Reply to comment by AxelBoldt in In Parkinson disease, why doesn't the adrenal gland fill the dopamine deficiency? by Actual-Pumpkin1567
Excellent question since, of course, the word can mean both. In this case, it is neurons which release dopamine. Note that they aren't just releasing it randomly into a tissue or into circulation, but releasing it directly at a targeted neuron, such as a GABA-releasing neuron of the dorsal striatum in a fine motor control circuit. A more comprehensive explanation of these pathways would probably require a smarter person to explain it.
BeneficialWarrant t1_j234w9l wrote
Reply to In Parkinson disease, why doesn't the adrenal gland fill the dopamine deficiency? by Actual-Pumpkin1567
Another way to think of it is that Parkinson's disease isn't a disorder of insufficient dopamine. Its a disorder of insufficient dopamine-releasing neurons. Treatment with dopamine precursors can increase the activity of remaining dopaminergic neurons of the SNpc. As the disease continues to progress, dopamine precursors become less effective.
BeneficialWarrant t1_j1nzrhf wrote
The amino acids interact with each other. The individual interactions are often very simple and involve such things as hydrogen bonding, acid/base salt bridges, hydrophobic exclusion, Van der Waals, sometimes covalent bonds such as disulfides.
While the interactions are simple, the sum of these interactions is very complex and significant. By changing the order that the amino acids are connected (and some other factors that are a bit more complex), the shape of the protein can be controlled.
The end result is a very large and bulky molecule with a very specific shape and that can interact with other molecules in very specific ways.
It's kinda like Legos. The individual bricks connect to each other in very simple ways, but a skilled builder with a plan can build a large creation with a very specific shape and function.
BeneficialWarrant t1_j0tzfdh wrote
Reply to comment by esach88 in Do babies see mirrors as focused or blurry? by Lord_Poopsicle
There isn't any evidence that looking at close up objects causes any permanent harm to eyes.
Losing the ability to focus on close up objects with aging (presbyopia) is just kinda one of those things that happens. The lens slowly becomes less stretchy (elastic) and won't fully snap back into a round shape when tension on it is released.
BeneficialWarrant t1_j0ru3a1 wrote
If you stand 12 inches in front of a mirror and focus on your own reflection, you are focusing your eyes to resolve an image that is 24" away. You can verify this by smearing a piece of toothpaste on your bathroom mirror. Focus on the toothpaste and your reflection will be out of focus.
BeneficialWarrant t1_jeguvs7 wrote
Reply to ELI5 how do animals know what to do when theyre born? by BruceToTheLee
If anything, behavior that is based so much on learning is the unusual outlier. In the animal kingdom, primates (and mammals in general) are strange for how much they have to learn. Its far more efficient to have neural circuits already designed for the skills you will need. The tradeoff is that we are incredibly adaptable to the environment and culture that we live in and can continue to add skills and nuance to our repertoire for many decades. I may not have been born knowing how to navigate the Sargasso Sea, but at least I could learn how to post comments on Reddit.